Overview
Painful progressive flatfoot, otherwise known as Tibialis Posterior Tendinitis, is caused by inflammation of the tendon of the tibialis posterior. The tendon then becomes inflamed, stretched or suffers a partial or total tear. If left untreated, this condition may lead to severe disability and chronic pain. Some people are predisposed to this condition if they have flatfeet or an abnormal attachment of the tendon to the bones in the midfoot. Nonsteroidal anti-inflammatory medications, ice, physical therapy, supportive taping and bracing, or orthotic devices are the common ways of treating painful progressive flatfoot. Contact your physician before taking any medication. In some cases, a surgical operation may need to be performed to repair the torn or damaged tendon and restore normal function. To prevent reinjury, orthotic devices may be recommended. In severe cases, surgery on the midfoot bones may be necessary to treat the associated flatfoot condition.
Causes
The most common cause of arch pain is plantar fasciitis. Plantar fasciitis is inflammation of the fibrous band of tissue that connects the heel to the toes. Sufferers of plantar fasciitis typically feel pain early in the morning when they first get out of bed. Another common cause of arch pain is fallen arches or flat feet. Fallen arches result in the sole of the foot becoming flat so that the entire sole of the foot touches the ground. Fallen arches can lead to pain in the ankles, knees, feet, and even in the legs. While fallen arches are often inherited, for some it develops as a result of wear and tear on your feet. Wearing shoes without proper metatarsal support, or arch support, can overstretch the tendon that supports the arch causing the arch to flatten out.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch.
Non Surgical Treatment
For mild pain or aching, acetaminophen (Tylenol) or a nonsteroidal anti-inflammatory drug (NSAID), such as aspirin or ibuprofen (Advil, Motrin and others) may be effective. When there are no symptoms, treatment is not needed. If a child older than age 3 develops symptoms, the doctor may prescribe a therapeutic shoe insert made from a mold of the child's foot or a corrective shoe. As an alternative, some doctors recommend store-bought arch supports. These appear to work as well as more expensive treatments in many children. With any conservative, nonsurgical treatment, the goal is to relieve pain by supporting the arch and correcting any imbalance in the mechanics of the foot. Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies.

Surgical Treatment
The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot.
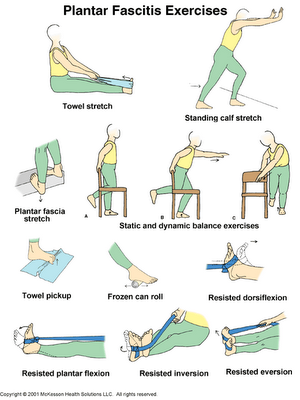
Stretching Exercises
Ankle evert or strengthening. Lie on your side with your feet hanging off the end of your bed or a weight bench. Bend the toes of the foot that is closer to the ceiling slightly toward your head. This is the starting position. Now raise your toes toward the ceiling while keeping the rest of your leg stationary. Return to the starting position. Reps. 10-15. Now point your toes slightly away from your head. This is the starting position. Raise your toes toward the ceiling. Return to the starting position. Reps. 10-15. Ankle invertor strengthening. Same as above, but do the exercises with the foot that is closer to the floor. Dorsiflexor strengthening. Sit on a desk, table, or counter so that your feet don?t touch the ground. Let your feet dangle comfortably. Bend your foot upward as far as you can comfortably go. Do not let your foot pull inward or outward. Return to the starting position. Reps. 10-15.
Painful progressive flatfoot, otherwise known as Tibialis Posterior Tendinitis, is caused by inflammation of the tendon of the tibialis posterior. The tendon then becomes inflamed, stretched or suffers a partial or total tear. If left untreated, this condition may lead to severe disability and chronic pain. Some people are predisposed to this condition if they have flatfeet or an abnormal attachment of the tendon to the bones in the midfoot. Nonsteroidal anti-inflammatory medications, ice, physical therapy, supportive taping and bracing, or orthotic devices are the common ways of treating painful progressive flatfoot. Contact your physician before taking any medication. In some cases, a surgical operation may need to be performed to repair the torn or damaged tendon and restore normal function. To prevent reinjury, orthotic devices may be recommended. In severe cases, surgery on the midfoot bones may be necessary to treat the associated flatfoot condition.
Causes
The most common cause of arch pain is plantar fasciitis. Plantar fasciitis is inflammation of the fibrous band of tissue that connects the heel to the toes. Sufferers of plantar fasciitis typically feel pain early in the morning when they first get out of bed. Another common cause of arch pain is fallen arches or flat feet. Fallen arches result in the sole of the foot becoming flat so that the entire sole of the foot touches the ground. Fallen arches can lead to pain in the ankles, knees, feet, and even in the legs. While fallen arches are often inherited, for some it develops as a result of wear and tear on your feet. Wearing shoes without proper metatarsal support, or arch support, can overstretch the tendon that supports the arch causing the arch to flatten out.
Symptoms
If you've ever seen your footprints in the sand and they looked more like bricks than feet, then you probably have flat feet. Simply stated, a flat foot is a foot that does not have an arch when standing. In the medical world, flat feet are associated with "pronated" feet. Pronated is merely the term used to describe the position of the foot when it is flexed upward (dorsiflexed), turned away from the body (abducted), and the heel is rolled outward (everted), all at the same time. A certain amount of pronation is required for normal walking, but too much pronation is often considered a foot's "worst enemy." Over time, excessive pronation can lead to many unpleasant problems including heel pain, bunions, hammertoes, shin splints, and even knee, hip, or back pain. In fact, one orthopedic surgeon discovered that 95% of his total knee replacement patients and 90% of his total hip replacement patients had flat feet. An easy way to tell if you pronate too much is to take a look at your athletic shoes-excessive wearing of the inside heel (arch side of the shoe) as compared to the outside is a classic indication of excessive pronation.
Diagnosis
The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch.
Non Surgical Treatment
For mild pain or aching, acetaminophen (Tylenol) or a nonsteroidal anti-inflammatory drug (NSAID), such as aspirin or ibuprofen (Advil, Motrin and others) may be effective. When there are no symptoms, treatment is not needed. If a child older than age 3 develops symptoms, the doctor may prescribe a therapeutic shoe insert made from a mold of the child's foot or a corrective shoe. As an alternative, some doctors recommend store-bought arch supports. These appear to work as well as more expensive treatments in many children. With any conservative, nonsurgical treatment, the goal is to relieve pain by supporting the arch and correcting any imbalance in the mechanics of the foot. Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies.
Surgical Treatment
The main goal of surgery is to reduce pain and improve function. It may also reduce other injuries such as repeated ankle sprains and broken bones. Surgery may be considered if there is no relief with physical therapy, changes in shoewear and/or changes in activity. Some patients will also have tendon problems, ankle weakness and foot fractures. These patients may require other procedures to address related problems. If you have medical problems that make surgery unsafe, any infections or blood vessel disease, cavus foot surgery may not be appropriate. The surgical procedures involved with the correction of the cavus foot are varied. Theses may include correction of the bony deformity, ankle looseness and the muscle imbalances that cause the deformity. The goal is to provide a foot that evenly distributes weight along both inside and outside edges. A variety of incisions may be needed to perform the procedures related to the correction of the cavus foot.
Stretching Exercises
Ankle evert or strengthening. Lie on your side with your feet hanging off the end of your bed or a weight bench. Bend the toes of the foot that is closer to the ceiling slightly toward your head. This is the starting position. Now raise your toes toward the ceiling while keeping the rest of your leg stationary. Return to the starting position. Reps. 10-15. Now point your toes slightly away from your head. This is the starting position. Raise your toes toward the ceiling. Return to the starting position. Reps. 10-15. Ankle invertor strengthening. Same as above, but do the exercises with the foot that is closer to the floor. Dorsiflexor strengthening. Sit on a desk, table, or counter so that your feet don?t touch the ground. Let your feet dangle comfortably. Bend your foot upward as far as you can comfortably go. Do not let your foot pull inward or outward. Return to the starting position. Reps. 10-15.
 RSS Feed
RSS Feed